
Case 55
Dr Marina-Portia Anthony / Professor Pek-Lan Khong
Clinical notes
An 11-year-old girl presented with a 3 month history of right knee pain and swelling. There was no history of trauma or fever.Images
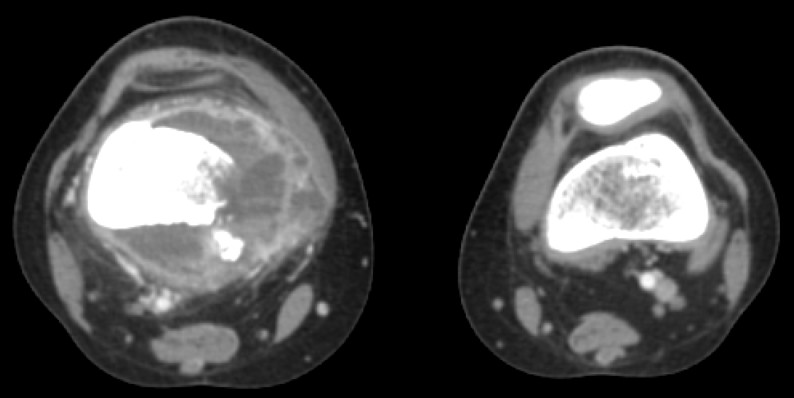

Figure 1.
Axial contrast-enhanced CT (A) and fused FDG-PET/CT (B) images through the distal femora.


Figure 2.
Reformatted coronal contrast-enhanced CT on bone algorithm (A) and fused FDG-PET/CT (B) images of the distal femora.
Show the video
References
- Adler LP, Blair HF, Makley JT, Williams RP, Joyce MJ, Leisure G, et al. Non-invasive grading of musculoskeletal tumours using PET. J Nucl Med. 1991 Aug;32(8):1508-12.
- Franzius C, Sciuk J, Daldrup-Link HE, Jürgens H, Schober O. FDG-PET for detection of osseous metastases from malignant primary bone tumours: comparison with bone scintigraphy. Eur J Nucl Med. 2000;27(9):1305-11.
- Lin EC, Alavi A. PET and PET/CT. 2005. Thieme Medical Publishers Inc. New York.
- Strobel K, Exner UE, Stumpe KD, Hany TF, Bode B, Mende K, et al. The additional value of CT images interpretation in the differential diagnosis of benign vs. malignant primary bone lesions with 18F-FDG-PET/CT. Eur J Nucl Med Mol Imaging. 2008;35(11):2000-8.
- Von Shulthess G. Molecular Anatomic Imaging. 2007.Lippincott Williams & Willkins. Philadelphia.