Dr Marina-Portia Anthony
Clinical notes
A 49 year-old man presented with 2 weeks of vague central abdominal pain and fever.
Images
Figure 1.
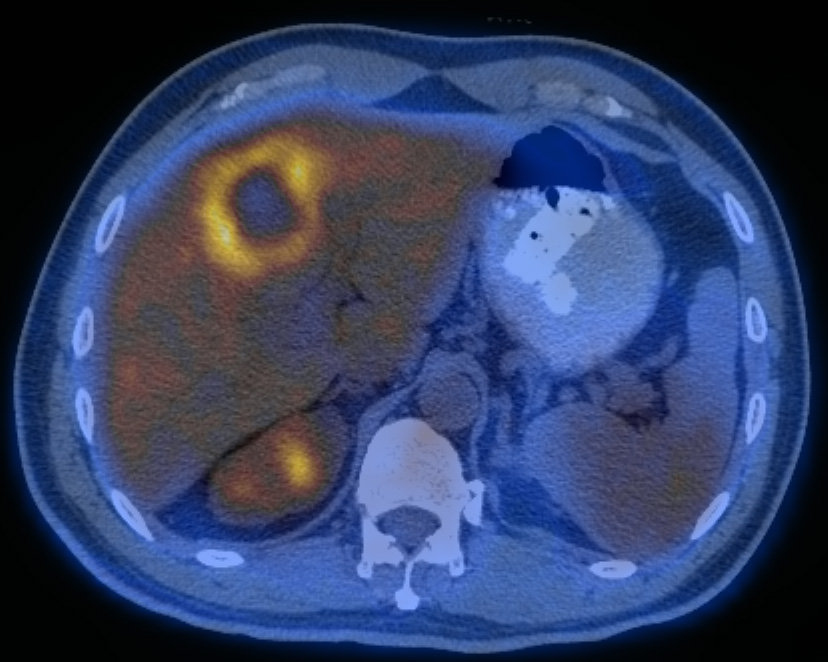
Axial non-contrast enhanced CT (A) and fused FDG-PET/CT (B) images of the upper abdomen.
Findings
In segment IVa of the liver, there is a large hypodense mass with an FDG-avid rim (SUVmax 4.2).
Diagnosis
Hepatic abscess. A culture grew Streptococcus milleri (anginosus).
Discussion
Most liver abscesses are pyogenic, resulting from a bacterial infection elsewhere. Organisms may reach the liver by: the portal vein, arterial supply, ascending infection in the biliary tract, direct invasion, or a penetrating injury. Immunosuppressed patients (eg old age with debilitating disease, immunosuppression, chemotherapy with marrow failure) may develop liver abscesses in the absence of infection elsewhere.
Clinically, liver abscesses may be associated with fever, right upper quadrant pain and tender hepatomegaly. Jaundice may occur if there is extrahepatic biliary obstruction. Whilst antibiotic therapy can be used for small abscesses, surgical drainage is often required for larger abscesses. Delayed diagnosis may occur due to frequent coexistent disease. The mortality rate for large liver abscesses is therefore high, ranging from 30% to 90%.
FDG-PET/CT significantly contributes to establishing a final diagnosis in patients with prolonged fever. Conversely, benign lesions such as due to infection or inflammation, are frequent causes (up to 25%) of false positive interpretation in PET/CT scans performed for proven or suspected malignancy. The CT component helps in morphologic characterization of lesions, and thereby increases the specificity of PET/CT, particularly for lesions with moderate or marked FDG uptake.
References
- Jaruskova M, Belohlavek O. Role of FDG-PET and PET/CT in the diagnosis of prolonged febrile states. Eur J Nucl Med Mol Imaging. 2006;33(8):913-8.
- Kumar V. Abbas A. Fausto N. Robbins and Cotran Pathologic Basis of Disease. 2005. Elselvier. Pennsylvania.
- Lin EC, Alavi A. PET and PET/CT. 2005. Thieme Medical Publishers Inc. New York.
- Metser U, Miller E, Lerman H, et al. Benign nonphysiologic lesions with increased 18F-FDG uptake on PET/CT: characterization and incidence. AJR Am J Roentgenol. 2007;189(5):1203-10.