
Case 4
Dr Marina-Portia Anthony /Dr Henry Mak
Clinical notes
A 65 year-old male patient presented with rising CEA, post-surgery and radiotherapy for rectal cancer, and post-chemotherapy for liver and lung metastases.Images

A.
Unenhanced axial CT image of the pelvis
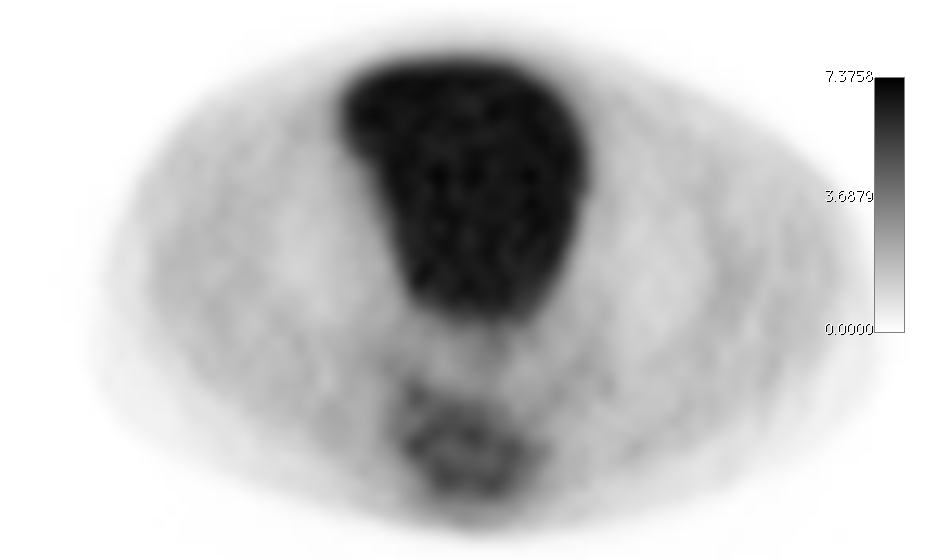
B.
Axial FDG-PET image of the pelvis
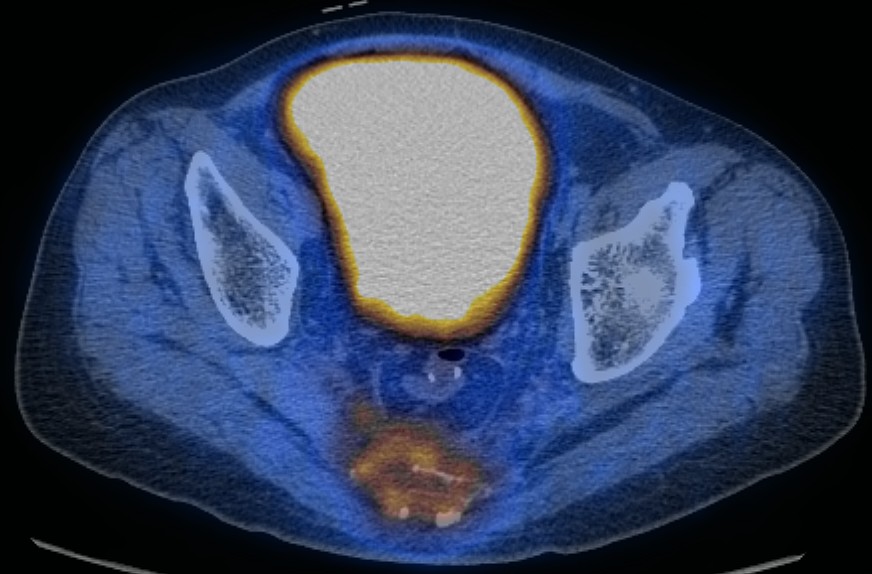
C.
Axial fused PET-CT image of the pelvis
References
- Bellomi M. Rizzo S. Travaini L. et al. Role of multidetector CT and FDG-PET/CT in the diagnosis of local and distant recurrence of resected rectal cancer. Radiol Med. 2007; 112(5): 681-90.
- Capirci C. Rampin L. Erba P. et al. Sequential FDG-PET/CT reliably predicts response of locally advanced rectal cancer to neo-adjuvant chemo-radiation therapy. Eur J Nucl Med Mol Imaging. 2007; 34(10): 1583-93.
- Kumar V. Abbas A. Fausto N. Robbins and Cotran Pathologic Basis of Disease. 2005. Elselvier. Pennsylvania.
- Schaefer O, Langer M. Detection of recurrent rectal cancer with CT, MRI and PET/CT. Eur Radiol. 2007; 17(8): 2044-54.
- Votrubova J. Belohlavek O. Jaruskova M. The role of FDG-PET/CT in the detection of recurrent colorectal cancer. Eur J Nucl Med Mol Imaging. 2006; 33(7): 779-84.